Categories
Change Password!
Reset Password!


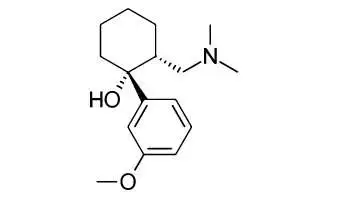
Tramadol is a centrally acting analgesic with a unique, dual mechanism of action, within the central nervous system (CNS). It exerts agonistic properties at opiate receptors and interferes with neurotransmitter reuptake.
Tramadol is a centrally acting analgesic with a unique, dual mechanism of action, within the central nervous system (CNS). It exerts agonistic properties at opiate receptors and interferes with neurotransmitter reuptake. Tramadol also binds weakly to µ-opiate receptors, blocking pain signal transmission to brain. Tramadol has been effective in controlling post-operative pain, but is not suitable as an adjunct to anesthesia because of low sedative properties.
Pharmacological Class: Opioid analgesic
Tramadol is a centrally-acting opioid analgesic. Although its mode of action is not completely understood, from animal tests, at least two complementary mechanisms appear applicable: binding of parent and M1 metabolite to μ-opioid receptors and weak inhibition of reuptake of norepinephrine and serotonin. Opioid activity is due to both low affinity binding of the parent compound and higher affinity binding of the O-demethylated metabolite M1 to μ-opioid receptors. The relative contribution of both tramadol and M1 to human analgesia is dependent upon the plasma concentrations of each compound. Tramadol is known to inhibit reuptake of norepinephrine and serotonin in vitro, as some other opioid analgesics. These mechanisms may contribute independently to the overall analgesic profile of tramadol.
Tramadol absorption is found to be 34% ±34. Volume of distribution is found to be 2.7 l/kg and plasma protein binding is 20%. Renal Excretion accounts for 30% (unchanged) 60% (as metabolite) and plasma half life is 6.3 hours.
Common (affecting between 1 in 10 to 1 in 100)
Uncommon (affecting 1 in 100 to 1 in 1000)
Very rare (affecting less than 1 in 10,000)










Comments (0)