Categories
Change Password!
Reset Password!


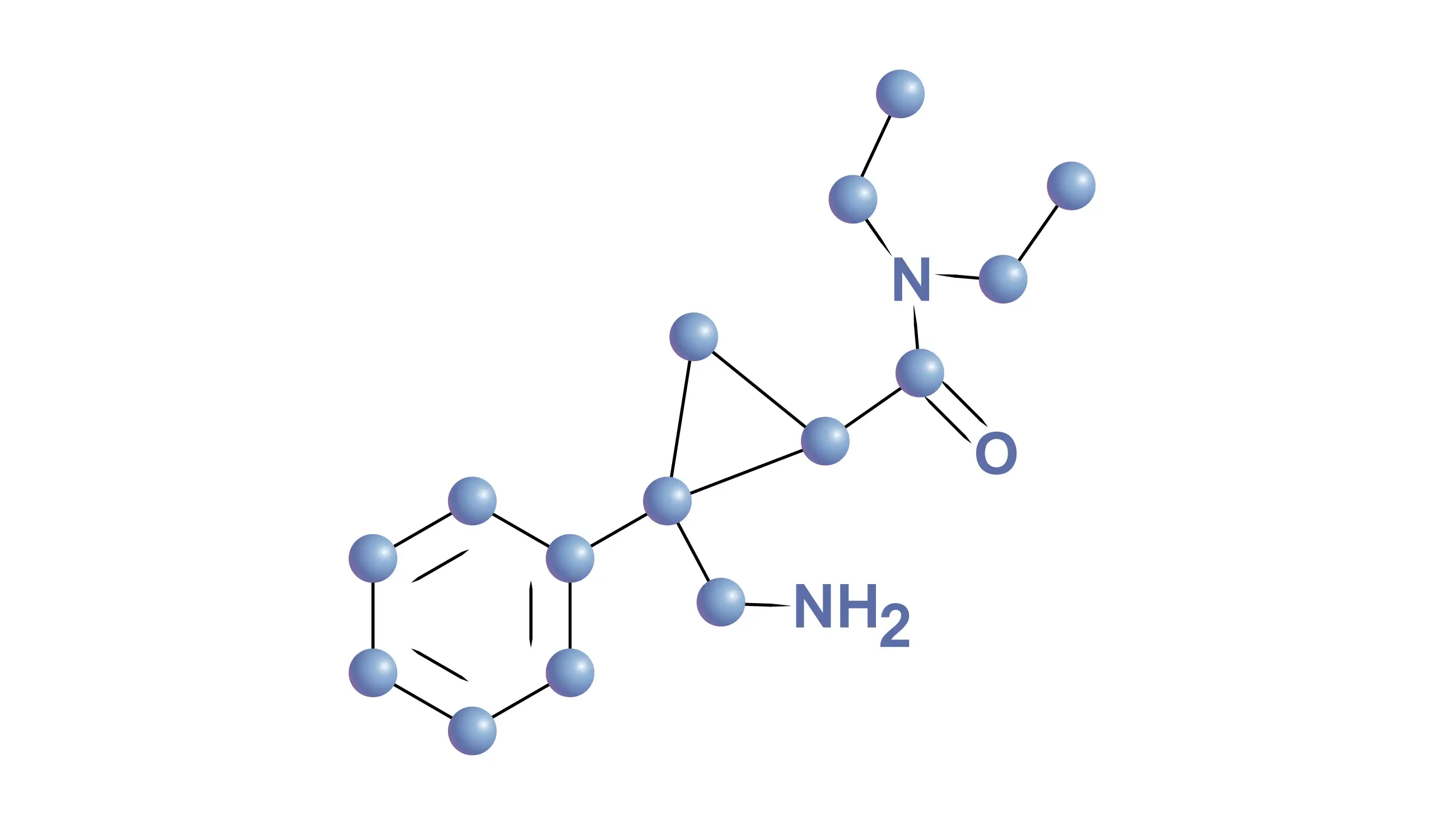
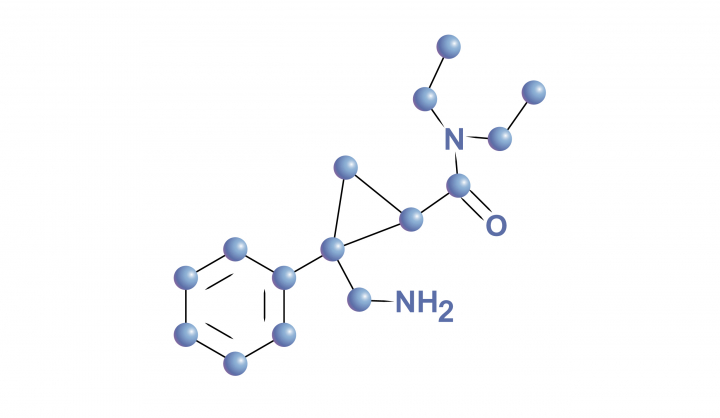
Milnacipran, a selective serotonin and norepinephrine reuptake inhibitor, is used to treat fibromyalgia and major depressive disorder in short term.
Milnacipran, a selective serotonin and norepinephrine reuptake inhibitor, is used to treat fibromyalgia and major depressive disorder in short term. It was given FDA approval in 2009 for fibromyalgia management. [1] It effectively decreases pain transmission and is suggested as first-line therapy for fibromyalgia. [2]
Pharmacological Class: Selective serotonin and norepinephrine reuptake inhibitors (SNRI) [1]
Milnacipran is indicated to alleviate fibromyalgia in people that are 18 years old and above. [3]
It is not approved for pediatric patients. [2]
Milnacipran has a mild affinity for inhibiting N-methyl-D-aspartate and blocks the reuptake of both serotonin and norepinephrine. [4] It exhibits three-fold better effectiveness for suppressing norepinephrine reuptake than serotonin, that differentiates it from the SNRIs, that are more serotonin active. [2] It is hypothesized that Milnacipran's ability to regulate abnormal serotonergic and noradrenergic pathways contributes to its therapeutic abilities, while its exact mechanism of action in fibromyalgia is uncertain.
Given that both neurotransmitters have an impact on pain regulation, norepinephrine's selectivity over serotonin hasn't yet proven to demonstrate a general therapeutic benefit. In vitro, Milnacipran has no substantial affinity for benzodiazepine, opiate, dopaminergic, serotonergic, or gamma-aminobutyric acid receptors. It does not impact dopamine reuptake. [4]
Absorption
Following oral administration, racemic Milnacipran has an absolute bioavailability of around 85 to 90 %. After an oral dose, the racemic drug reaches its maximum concentrations in 2 to 4 hours, and steady-state levels are attained in 36 to 48 hours. Contrarily, Levomilnacipran exhibits a relative bioavailability of 92%.
Levomilnacipran's median time to peak concentration (Tmax) occurs 6 to 8 hours following oral treatment. Notably, 5196 ng/h/mL is the mean steady-state area under the curve value while the mean Cmax value is 341 ng/mL following daily administration of 120 mg of levomilnacipran. In general, taking levomilnacipran or racemic Milnacipran with meals has little effect on how well the drug is absorbed orally.
Volume of distribution
After giving healthy patients a single intravenous dosage of racemic Milnacipran, the mean volume of distribution was about 400 L. Levomilnacipran, on the other hand, has an extensive distribution with an apparent volume of distribution of 387–473 L.
Protein binding
For racemic Milnacipran, protein binding of 13% has been reported. In contrast, spanning a concentration range of 10 to 1000 ng/mL, levomilnacipran has been shown to bind plasma proteins at a rate of 22%.
Metabolism
Levomilnacipran is known to be converted into desethyl levomilnacipran and p-hydroxy-levomilnacipran, by desethylation and hydroxylation, respectively. For formation of conjugate Milnacipran carbamoyl-O-glucuronide, both oxidative metabolites are further conjugated with glucuronide. Desethylation is largely catalyzed by Cytochrome P450 3A4 (CYP3A4), with CYP2C8, 2C19, 2D6, and 2J2 minor contributions. It is generally accepted that there is no interconversion of Milnacipran's enantiomers within the body.
Route of elimination
Renal excretion is the main route by which levomilnacipran and its metabolites are removed. Approximately 58% of the dosage of 14C-levomilnacipran solution taken orally is eliminated in the urine as unaltered levomilnacipran. The primary metabolite excreted in the urine, which made up around 18% of the dosage, is N-desethyl levomilnacipran. p-hydroxy levomilnacipran (1% ), p-hydroxy levomilnacipran glucuronide (1%), desethyl levomilnacipran glucuronide (3%), and levomilnacipran glucuronide (4%) are other recognizable metabolites discharged in the urine.
Half-life
While d-Milnacipran exhibits a longer elimination half-life (8 to 10 hours) in comparison with the l–enantiomer (4 to 6 hours), the terminal elimination half-life of racemic Milnacipran has been documented to be 6 to 8 hours. The terminal elimination half-life was calculated particularly for levomilnacipran formulations, and it is around 12 hours.
Clearance
Milnacipran's total plasma clearance was estimated to be 40 L/h. [1]
The most commonly reported adverse effects are:
Efficacy, safety, and tolerability of Milnacipran for fibromyalgia management
Milnacipran was discovered to be safe, well-tolerated and efficient for the treatment of various fibromyalgia symptoms in a 27-week, randomized, double-blind, multicenter research done by Philip J. Mease. Placebo, 100 mg/day Milnacipran, and 200 mg/day Milnacipran were administered to 888 patients in total. Remarkable pain decreases were noted following week 1 with both 100 mg/day and 200 mg/day doses of Milnacipran. At 15 weeks, 200 mg/day of Milnacipran elicited substantial improvements over placebo in pain, patient global impression of change (PGIC), cognition, fatigue, and multiple Short Form-36 (SF-36) domains. [2,5]
According to a double-blind, placebo-controlled trial, a 100 mg/day dose of Milnacipran monotherapy was found to be effective in treating fibromyalgia patients' pain, exhaustion, global status, and overall physical and mental health. Overall, 1025 participants were randomly assigned to receive either a placebo (n = 509) or Milnacipran (n = 516) at a dose of 50 mg twice a day (100 mg/day). After 12 weeks, a considerably higher percentage of milnacipran-treated subjects versus placebo-treated subjects displayed remarkable improvements, as indicated by the percentage of individuals fulfilling the two-measure composite responder criteria (decreased pain and improved global status) and three-measure composite responder criteria (decreased pain, improved global status, and improved physical function). [2,6]
Another research was conducted to assess how long-term Milnacipran therapy affected fibromyalgia patients. This lengthy, open-label research enrolled 1227 patients who had completed a prior Milnacipran investigation. Patients with fibromyalgia who took Milnacipran for up to 3.25 years had long-lasting symptom improvements. No novel safety concerns were detected. [2,7]
. Milnacipran. Drug Bank. Accession Number DB04896. Available online from: https://go.drugbank.com/drugs/DB04896
[Last accessed on: 08 July 2022]
2. Gupta H, Girma B, Jenkins JS, Kaufman SE, Lee CA, Kaye AD. Milnacipran for the Treatment of Fibromyalgia. Health Psychol Res. 2021 Jul 10;9(1):25532.
3. Milnacipran. FDA LABEL. Available online from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2011/022256s011lbl.pdf
[Last accessed on: 08 July 2022]
4. English C, Rey JA, Rufin C. Milnacipran (Savella), a treatment option for fibromyalgia. Pharmacy and Therapeutics. 2010 May;35(5):261-6.
5. Mease PJ, Clauw DJ, Gendreau RM, Rao SG, Kranzler J, Chen W, Palmer RH. The efficacy and safety of milnacipran for treatment of fibromyalgia. a randomized, double-blind, placebo-controlled trial. The Journal of rheumatology. 2009 Feb 1;36(2):398-409.
6. Arnold LM, Gendreau RM, Palmer RH, Gendreau JF, Wang Y. Efficacy and safety of milnacipran 100 mg/day in patients with fibromyalgia: Results of a randomized, double‐blind, placebo‐controlled trial. Arthritis & Rheumatism. 2010 Sep;62(9):2745-56.
7. Arnold LM, Palmer RH, Ma Y. A 3-year, open-label, flexible-dosing study of milnacipran for the treatment of fibromyalgia. The Clinical Journal of Pain. 2013 Dec 1;29(12):1021-8.









Comments (0)