Categories
Change Password!
Reset Password!


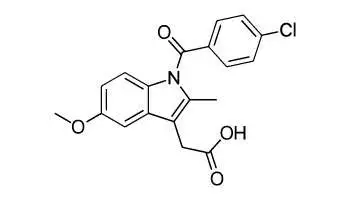
Indomethacin is a nonsteroidal anti-inflammatory drug (NSAID). Indomethacin works by reducing hormones that cause inflammation and pain in the body.
Indomethacin is a nonsteroidal anti-inflammatory drug (NSAID). Indomethacin works by reducing hormones that cause inflammation and pain in the body. It is used to treat moderate to severe osteoarthritis, rheumatoid arthritis, gouty arthritis, or ankylosing spondylitis. It is also used to treat shoulder pain caused by bursitis or tendinitis.
Pharmacological Class: NSAID
Indomethacin is a prostaglandin G/H synthase (also known as cyclooxygenase or COX) inhibitor that acts on both prostaglandin G/H synthase 1 and 2 (COX-1 and -2). Prostaglandin G/H synthase catalyzes the conversion of arachidonic acid to a number of prostaglandins involved in fever, pain, swelling, inflammation, and platelet aggregation. Indomethacin antagonizes COX by binding to the upper portion of the active site, preventing its substrate, arachidonic acid, from entering the active site.
Adult dose: 50 to 200 mg orally in divided doses with food
Pediatric dose: 1 mg/kg orally with 8 hour frequency
Note: Drug should not be given to pediatrics, pregnant mothers, patients suffering from liver malfunction, and neonates.
Oral absorption of Indomethacin is found to be 50% ±50. Volume of distribution is found to be 1 l/kg and plasma protein binding is 90-99%. Presystemic metabolism is noted to be 45.5% ±4.5 and metabolism is reported hepatic (extensive). Renal Excretion accounts for 60% and plasma half life is 1-16 hr.
Common (affecting between 1 in 10 to 1 in 100)
Uncommon (affecting 1 in 100 to 1 in 1000)
Very rare (affecting less than 1 in 10,000)










Comments (0)