Categories
Change Password!
Reset Password!


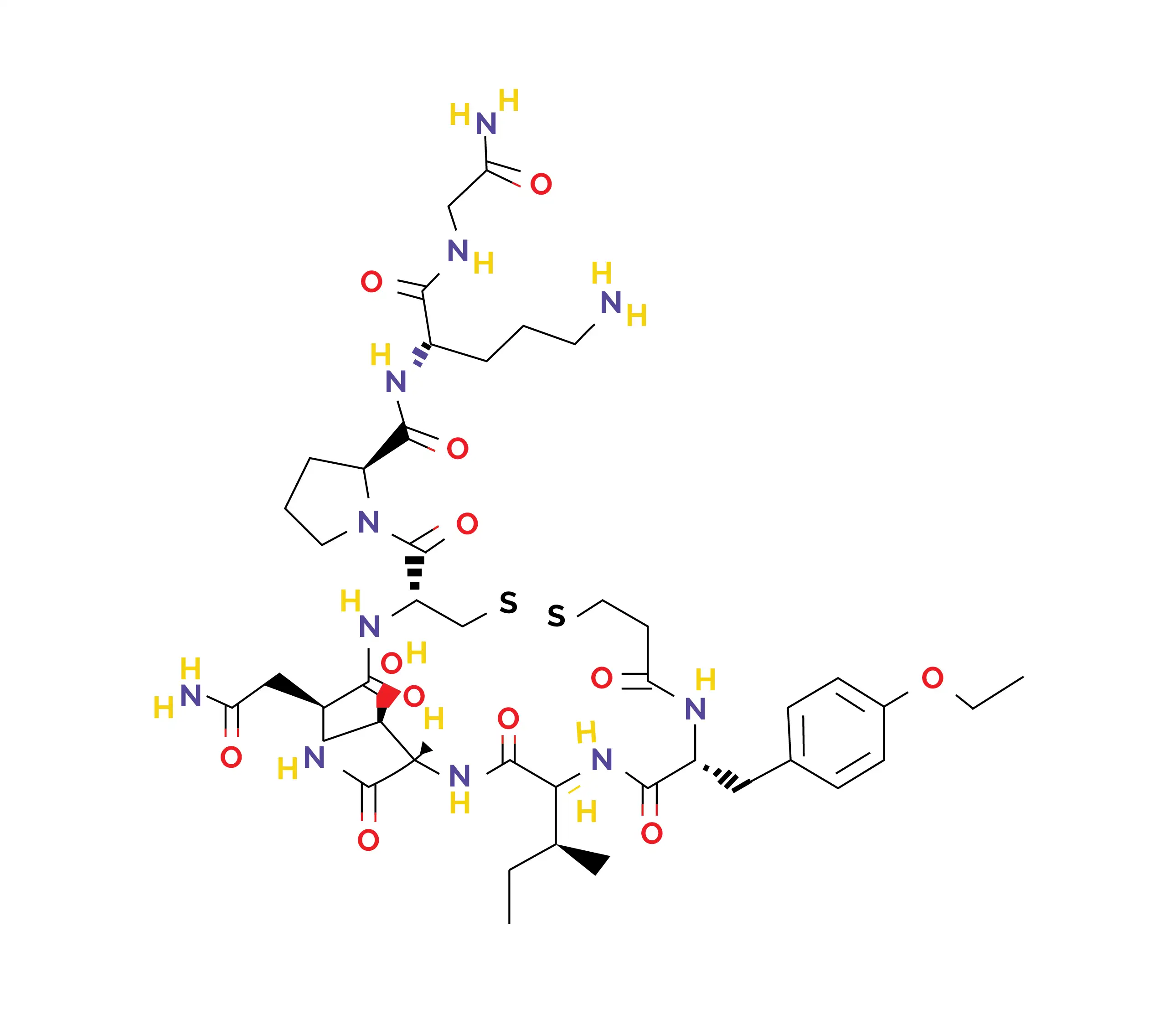
Atosiban is an oligopeptide that inhibits the hormones oxytocin and vasopressin.
Atosiban is an oligopeptide that inhibits the hormones oxytocin and vasopressin. It is administered intravenously to prevent premature or preterm labor (labor that arises prior to 37 weeks of gestation). [1, 2] It is available in both proprietary and generic forms and is approved for the management of imminent preterm birth in pregnant women displaying specific clinical observations. [2]
Chemical formula: C43H67N11O12S2
Atosiban is indicated for delaying imminent preterm birth in pregnant women who exhibit the following:
(a) Regular contractions of the uterus persisting for a minimum of 30 seconds, occurring at a rate of four or more times within 30 minutes
(b) Cervical dilation of 1-3 cm (0-3 cm for women who have never given birth) and at least 50% effacement (thinning and shortening of the cervix that occurs during pregnancy in preparation for childbirth)
(c) A gestational age of 24 to 33 completed weeks
(d) A normal fetal heart rate [2]
Atosiban may be used for ameliorating the success of in vitro fertilization-embryo transfer (IVF-ET). [3] It is particularly recommended for older and obese women facing repeated implantation failures during fresh embryo transfer cycles. [4]
The oxytocin system, which operates through uterine oxytocin receptors, is fundamental for human parturition. Raised levels of oxytocin receptors play a key role in commencing preterm labor. Atosiban, an oxytocin analog, has amino acid modifications at 1, 2, 4, and 8 positions. It competes with oxytocin for binding at these receptors, leading to a reduction in myometrial contractions. [5]This prevents oxytocin-triggered rises in inositol triphosphate levels, which is responsible for stimulating contractions.
This action, in turn, averts stored calcium release from the sarcoplasmic reticulum and the opening of voltage-sensitive calcium channels. As a result, the rise in cytosolic calcium is curtailed, preventing uterine muscle contractions, reducing their frequency, and inducing a state of uterine quiescence (state of the uterus where there are no coordinated contractions). Recent investigations have documented that atosiban also acts as a ligand exhibiting bias at oxytocin receptors. It serves as an antagonist of Gq coupling, which accounts for its inhibition of the inositol triphosphate pathway believed to mediate its effects on uterine contractions.
Conversely, atosiban acts as an agonist of Gi coupling, leading to a pro-inflammatory response in the human amnion by activating the pro-inflammatory signaling transducer nuclear factor kappa B (NF-κB). This pro-inflammatory activity is thought to diminish atosiban's efficiency when compared to other agents that do not induce inflammation, as inflammatory mediators are known to contribute to labor induction. [2] When used in cases of premature labor, atosiban quickly suppresses uterine contractions. Within 10 minutes of administration, it markedly decreases contractile activity, aiding to maintain a stable state of functional rest in the uterus for up to 12 hours. [6]
Atosiban is administered without any delay once the diagnosis of "preterm labor" is made.
Additional Considerations:
Absorption
Distribution
Metabolism
Excretion
(a) For management of preterm labor and preterm birth
A prospective multicentric research explored atosiban's efficiency and safety in 406 pregnant women diagnosed with preterm labor. The findings revealed that 89% of patients experienced prolonged gestation beyond 48 hours, with a mean prolongation of 31.28 days and an average delivery gestational age of 35 weeks. The 72-hour undelivered rate was 83.75%. In 77% of volunteers, preterm birth was delayed for more than 7 days. Adverse effects were minimal, including nausea (2.71%), tachycardia (2.46%), and headache (1.97%). Atosiban also curtailed the need for neonatal intensive care unit (NICU) admission, leading to substantial cost savings related to hospitalization. [5]
A prospective single-center study recruited 50 women experiencing preterm labor symptoms. Atosiban was administered as a 0.9 ml bolus. This was accompanied by 300 mcg/min infusion for two hours, then 100 mcg/min for twelve hours, using three 5 ml vials. The mean delay in delivery was found to be 18.13 ± 17.97 days (range 1-62 days). At 48 hours, 70% of women remained undelivered, and 58% remained undelivered at 7 days. Importantly, no adverse events for mothers and infants were documented. This brief atosiban regimen demonstrated a favorable safety and efficacy profile, facilitating ease of administration and leading to shorter healthcare facility stays. This change benefited both patients and clinical staff. Additionally, the overall cost of the therapy was reduced. [8]
Al-Riyami N and other investigators carried out a retrospective study to determine atosiban's effectiveness in delaying delivery in 159 pregnant women experiencing threatened preterm labor. As found, atosiban successfully delayed delivery by at least 48 hours in 130 cases (81.8%). Notably, about 50.9% of women achieved uterine quiescence within 12 hours. Adverse effects were minimal, with only 9.4% of women experiencing minor side effects. In conclusion, atosiban proved highly useful in delaying delivery with minimal adverse maternal and neonatal outcomes. [9]
In a trial by Romero R and colleagues, 531 pregnant women in preterm labor were randomized to get either intravenous atosiban (n = 246) or placebo (n = 255), followed by subcutaneous maintenance. Atosiban treatment prolonged pregnancy for up to 7 days in patients ≥28 weeks gestational age, with a favorable safety profile. [10]
(b) For prevention of premature delivery in twin pregnancies
In a retrospective study by Mariavittoria L et al. involving 202 women with twin pregnancies and threatened preterm labor, the effectiveness of atosiban was investigated. Among 98 women receiving a single cycle of atosiban, 34% delivered before 34 weeks. A second cycle was administered to 104 patients with ongoing contractions or cervical changes before 32 weeks (Group A). Notably, 49 of these patients also received vaginal lactoferrin tablets (Group B).
After the second cycle, 84% in Group A and 90% in Group B delivered after 34 weeks. Overall, the rate of delivery before 34 weeks was only 16% in the study groups. Repeated atosiban cycles effectively delayed delivery in twin pregnancies, supporting its use as a first-line therapy, especially given the elevated risk of pulmonary edema in these cases. [11]
(c) For improving pregnancy outcomes in women with IVF implantation failures
In a systematic review and meta-analysis by Wang R and colleagues, atosiban improved pregnancy outcomes in repeated embryo implantation failure patients undergoing IVF-ET. Overall, 7 studies, including 2 randomized controlled trials, 1 prospective cohort, and 4 retrospective cohort studies, were analyzed. Atosiban was linked to a remarkably higher clinical pregnancy rate (Risk Ratio [RR]=1.54). The findings of subgroup analyses indicated a higher clinical pregnancy rate in the atosiban group across all study types and regardless of whether participants had 2 or 3 previous embryo transfer failures. There were no vital differences in ectopic pregnancies, multiple pregnancies, or miscarriages between the study and control groups. [3]
A retrospective cohort study recommended atosiban for older and obese women experiencing repeated implantation failures during fresh embryo transfer cycles, especially with cleavage-stage embryos. As found, atosiban improved clinical pregnancy rates in women with more than three embryo transfer cycles (Odds Ratio [OR] 1.667), particularly in those aged 35 or older (OR 1.851), obese women (OR 2.550), and with cleavage-stage embryos (OR 1.721). Atosiban also boosted live birth rates in obese women. [4]













Comments (0)