Categories
Change Password!
Reset Password!



A study was carried out to investigate early surgery and delayed surgery in terms of the occurrence of residual choledocholithiasis and the readmission rate for recurrent biliary events.
Early cholecystectomy lowers the readmission rate for biliary events, presence of residual choledocholithiasis, and the need for endoscopic retrograde cholangiopancreatographies in people with acute biliary pancreatitis.
A study was carried out to investigate early surgery and delayed surgery in terms of the occurrence of residual choledocholithiasis and the readmission rate for recurrent biliary events.
In this multicentric randomized clinical trial, 198 subjects with mild acute biliary pancreatitis were examined and randomized into two groups (i) Early surgery group (n=98) where cholecystectomy was performed after a week, and (ii) Delayed surgery group (n=100) where cholecystectomy was performed after 4 weeks. For excluding persistent choledocholithiasis, intraoperative or preoperative imaging was carried out in all the subjects.
Early surgery lowered the readmission rate for biliary events prior to cholecystectomy by half. The percentage of people reporting choledocholithiasis is shown in Table 1:
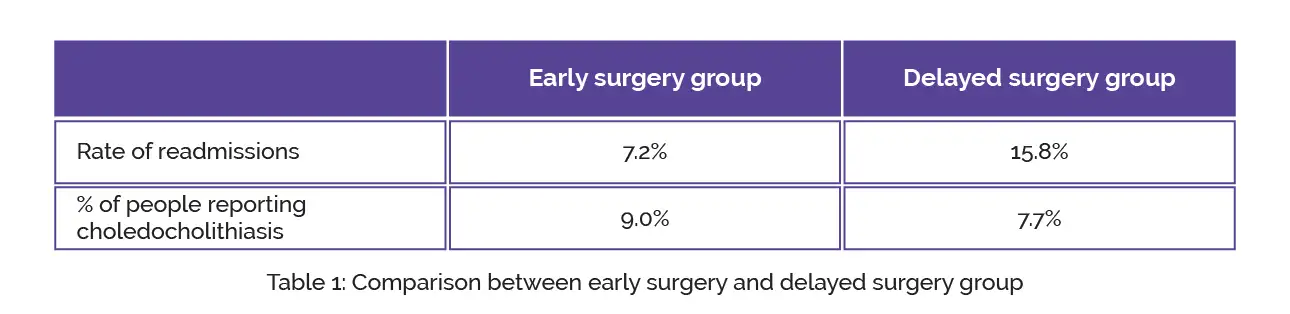
No differences were reported in the complications, postoperative stay, type of surgery when compared with delayed surgery. The intraoperative or preoperative imaging study resulted in avoidance of unwanted endoscopic retrograde cholangiopancreatographies (ERCP), which was carried out in only 6 (3%) people.
Early cholecystectomy conducted a week after mild acute biliary pancreatitis showed a reduced occurrence of complications and recurrent biliary events, and was not related to a rise in residual choledocholithiasis or requirement for unnecessary ERCP.
International Journal of Surgery
Cholecystectomy 7 days vs 4 weeks after mild biliary pancreatitis; looking a decrease the incidence of persistent choledocholithiasis and ERCP: A multicentric randomized clinical trial.
Helena Gómez Facundo et al.











Comments (0)