Categories
Change Password!
Reset Password!



One of the most prevalent musculoskeletal conditions and a key contributor to disability globally is neck pain or cervicalgia.
The use of longwave diathermy for 2 weeks is an efficient therapeutic strategy to improve neck pain, neck range of motion (neck extension), and neck disability.
One of the most prevalent musculoskeletal conditions and a key contributor to disability globally is neck pain or cervicalgia. As per the Global Burden of Disease 2010 survey, neck pain is the fourth most commonly reported reason for years of disability. In the adult population (age 15 to 74 years), the neck pain prevalence ranges from 5.9% to 38.7%. In comparison to men, women are highly likely to experience cervicalgia.
On the basis of the length, mechanism, etiology etc, neck pain has been divided into several categories. Depending on how long it lasts, neck pain can be classified as acute (lasting less than six weeks), subacute (lasting ≤ three months), or chronic (lasting longer than three months). Based on mechanism, neck pain may be divided into mechanical and neuropathic types. It may also be divided into two categories based on the type of cause, namely primary and secondary. Mechanical neck pain exhibits an insidious nature. It has many contributing factors, such as physical and occupational activity, depressive disorders, anxiety, bad posture, and neck strain.
On the other hand, neuropathic pain is a form of pain that is elicited by any disease or injury affecting the peripheral nervous system. Studies have shown that the osseo-ligamentous system, that offers stabilization primarily at the end range of posture, contributes 20% of the mechanical stability of the cervical spine. On the other hand, dynamic support is offered by muscles in activities in neutral-range and mid-range postures.
The therapy majorly incorporates conservative and surgical intervention. Exercises including stretching and strengthening routines, exercises done at home, and cervical collars make up conservative therapy. Spinal manipulation, soft cervical collars, traction, exercise, massage therapy, acupuncture and electrotherapy techniques like longwave diathermy, ultrasonic therapy, shortwave diathermy, interferential therapy, and transcutaneous electrical nerve stimulation are among the additional physiotherapy approaches.
Cervical fusion and cervical decompression are included in surgical treatments. Research has shown that they exhibit better effects than anterior cervical decompression and cervical replacement. Capacitive and resistive electric transfer treatment, or longwave diathermy, is a sort of heating electrotherapeutic method that increases the microcirculation and metabolic flow of the superficial and deep tissues while also producing heat.
Diathermy, which means "through heating," is the process of heating the tissues in between two electrodes. High-frequency currents with 1,000,000-3,000,000 cycles per second are employed by diathermy for heat generation. Longwave diathermy operates at frequencies between 0.3 and 1 MHZ and a wavelength of 300 m. The longwave diathermy penetration range is as deep as 2 inches. Longwave diathermy produces electromagnetic fields that oscillate and contain both magnetic and electric fields.
Because of the rapid alternating movement of ions caused by these fields, heat is produced in the tissues. The blood vessels and muscles are heated by the longwave diathermy at the molecular level. Owing to the insulating effects of fat tissues, the heat that is produced gets retained. The physiological benefits of longwave diathermy incorporate a relaxation of muscular spasms, a decline in tissue stiffness, an improvement in range of motion, a rise in deep tissue temperature, an elevation in metabolic activity, and a decrease in pain.
The longwave diathermy equipment consists of a treatment head and a cream designed specifically for longwave diathermy that is put between the afflicted area and the treatment head as a coupling medium. Capsulitis, bursitis, tendinitis, rheumatoid arthritis, osteoarthritis, and other disorders are among the most frequent ones for which longwave diathermy is prescribed. Additionally, it can be utilized to relieve the pain brought on by ailments including neuralgia, kidney stones, muscular spasms, and sinusitis.
Pelvic inflammatory disease is a significant additional indicator. But, it is contraindicated in regions of anesthesia, pus-filled lesions, arteriosclerosis, and cancer. Numerous studies have examined the impact of longwave diathermy on various conditions. One trial that looked at the influence of longwave diathermy and myofascial release (MFR) on upper trapezius spasm came to the conclusion that the results were adequate.
In a prior trial, longwave diathermy was contrasted with groups getting a manual massage and sham longwave diathermy to treat delayed onset of muscle soreness in athletes. No clinical differences were witnessed in numeric pain rating scale (NPRS), whereas, there were few variations in Patient Global Impression Scale. A comparative study was also conducted to examine the efficacy of longwave diathermy and MFR vs. ultrasound therapy and MFR for treating plantar fasciitis pain in patients, and the findings showed that longwave diathermy and MFR were somewhat more successful than ultrasound therapy.
RATIONALE BEHIND RESEARCH
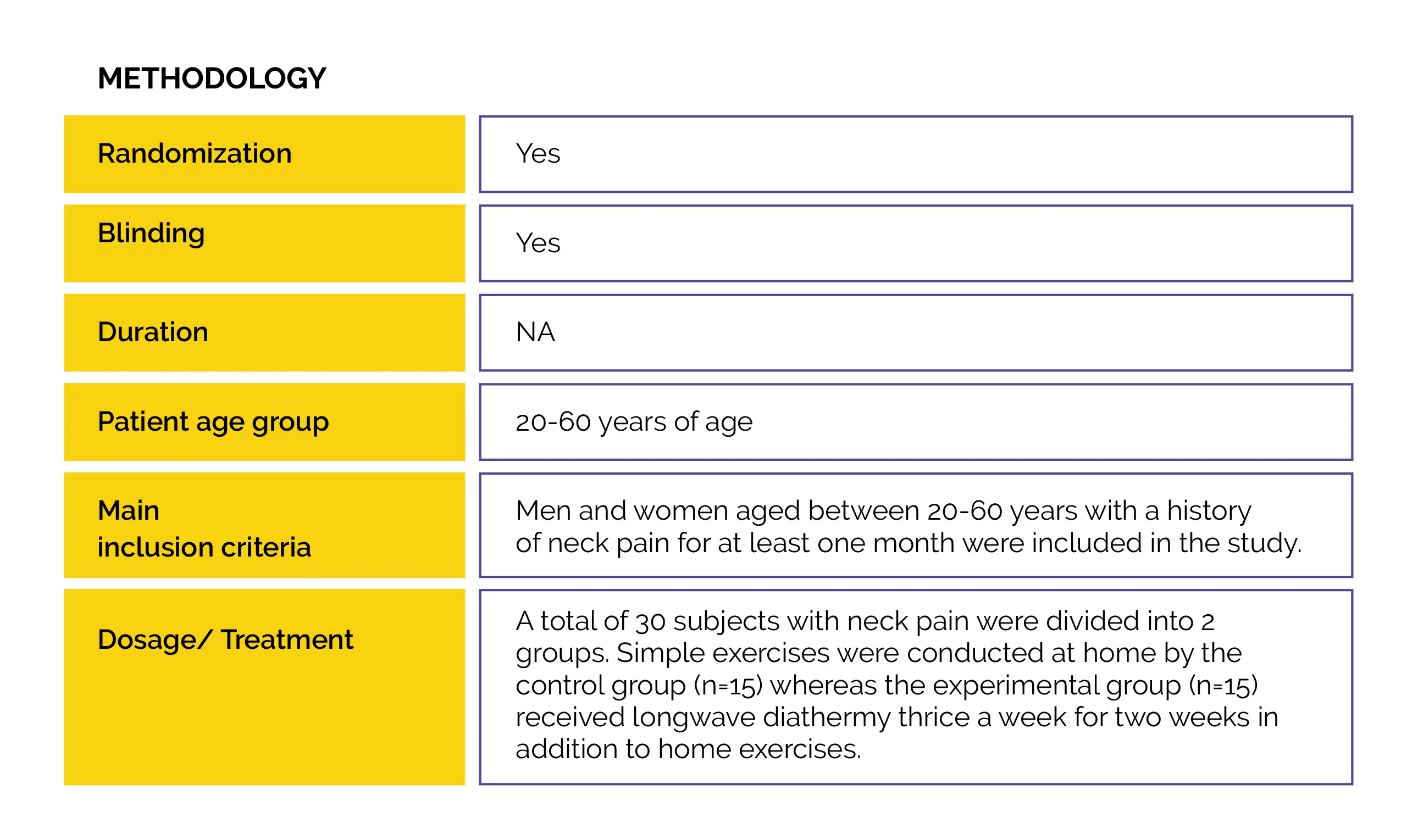
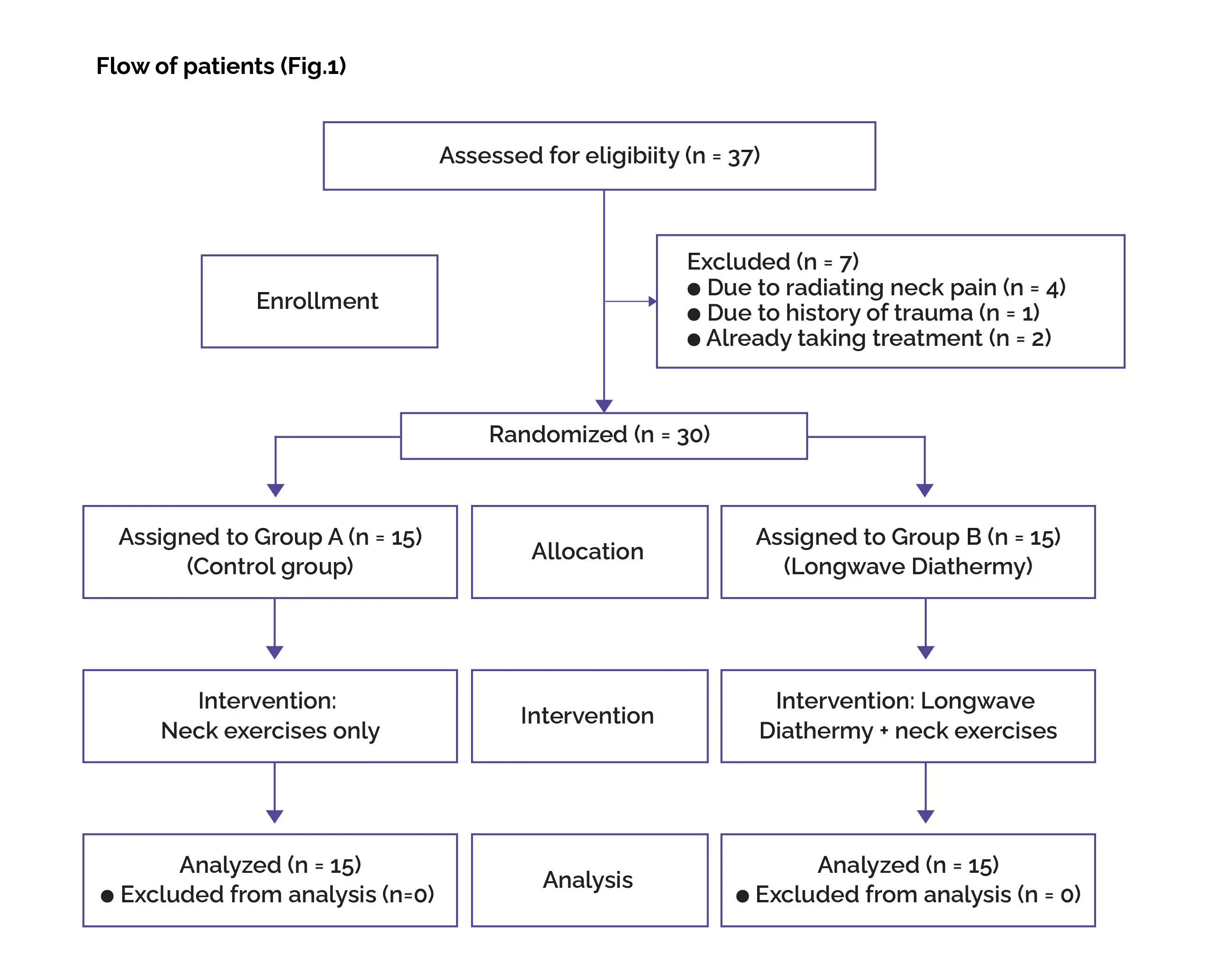
A wide array of therapies for treating neck pain and its accompanying symptoms have been studied. But, there is little research on how longwave diathermy affects neck pain and impairment. Therefore, this single-blinded, participant-blinded, randomized controlled trial was carried out.
OBJECTIVE
The objective of this study was to investigate the efficacy of longwave diathermy for the management of neck pain.
Study outcomes
At baseline, at the end of two weeks (post-intervention), and post-follow-up of 2 weeks, the outcomes ascertained were visual analogue scale (VAS), neck disability index (NDI), and neck range of motion.
Outcomes
Baseline: There were no vital differences reported at baseline.
Study outcomes
In this study, the effectiveness of longwave diathermy was determined in individuals with neck pain in terms of their neck range of motion, disability, and neck pain. When pre and post-intervention readings were contrasted, the study's findings showed that there was a profound enhancement among the members of the control group (Group A) for all outcome measures, like neck disability, neck range of motion, and pain with the exception of neck side flexion to the right side.
Pre and post-treatment readings showed a substantial betterment in all of the outcome measures in the experimental group (Group B), which underwent longwave diathermy as an intervention coupled with neck exercises. Additionally, there was a substantial difference between the pre-intervention and post-intervention readings, indicating that the enhancement from the provided intervention persisted during the follow-up period.
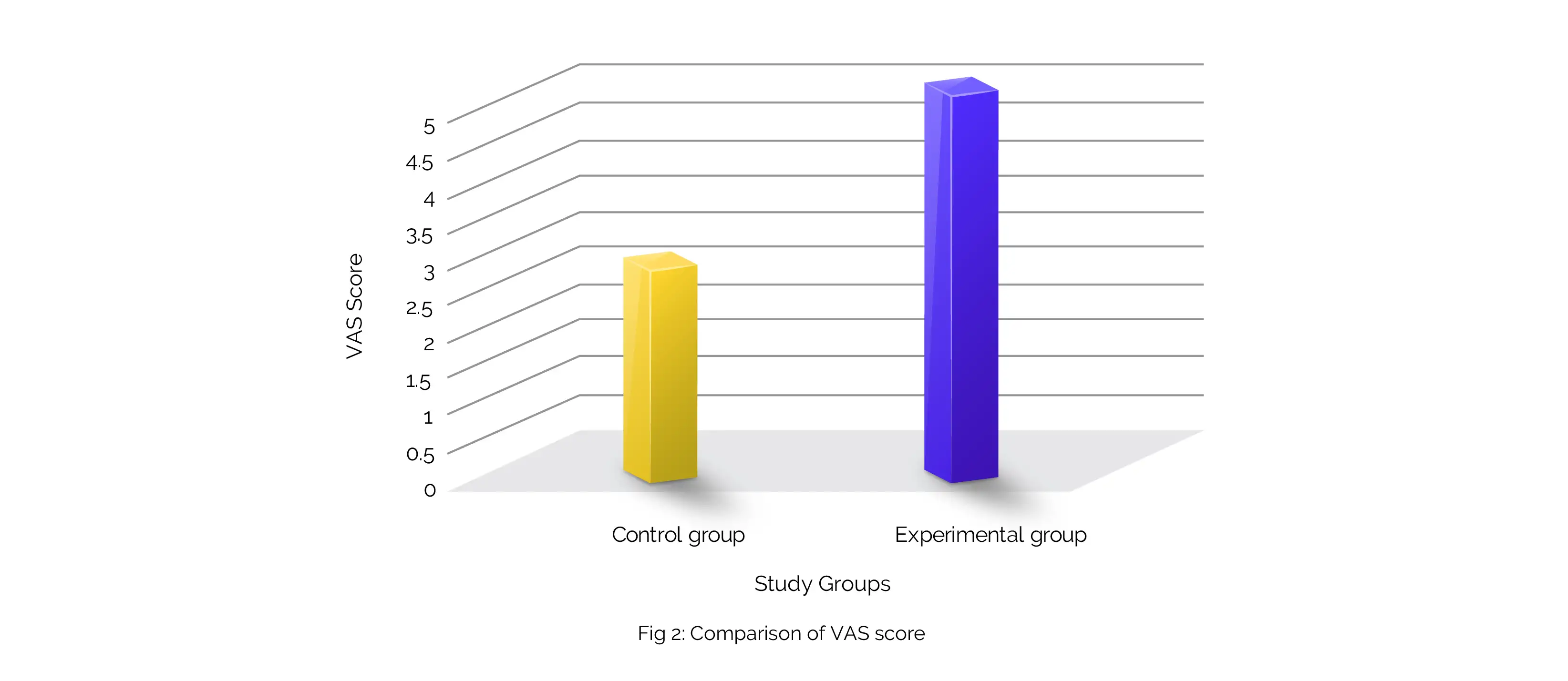
For the neck extension range of motion, NDI, and VAS, the intergroup comparison revealed that the longwave diathermy group experienced a greater improvement when compared to the control group. However, no variation was seen between the groups for neck rotation to either side, side flexion, or neck flexion. The findings of the current investigation are consistent with a previous study carried out on subjects who had upper trapezius muscular spasms. The upper trapezius muscle spasm improved when longwave diathermy was applied constantly for six days.
The findings of the research are supported by another research that comprised 3 groups of patients with neck pain, back pain, and frozen shoulder. In this study, the use of longwave diathermy reduced VAS readings. More trials have been carried out using longwave diathermy on distinct body parts. In an investigation by Manigandan and Sangeetha, longwave diathermy (three times/week) was used in patients with plantar fasciitis. According to the results, after four weeks of treatment, there was a significant decrease in pain and an improvement in foot functioning.
Another trial on delayed onset of muscle soreness found no clinically meaningful difference between the 10-minute single-sit application of sham longwave diathermy and longwave diathermy in terms of NPRS in ski-mountaineering racers. The one-time use of longwave diathermy might be the cause of the non-significant change. The activation of cutaneous thermoreceptors, which results in the creation of heat and the restriction of the transmission of pain when it enters the corresponding area of the spinal cord through the pain gate mechanism, may have contributed to the decrease of pain in the longwave diathermy patients.
The peripheral nerves' increased nerve conduction velocity brought on by heat aids the pain-relieving process even more. Longwave diathermy's heat also triggers chemicals associated with pain mediation, such as bradykinin, serotonin, and prostaglandins, to vasodilate and efflux from the damaged tissue. A rise in microcirculation and metabolism is also stimulated by heat. Pain relief also adds to the reduction in neck impairment and improvement in functionality.
Various studies that have been conducted to ascertain the impact of exercises on the range of motion, disability, and neck pain may help to explain the betterment in the range of motion, disability, and neck pain in the control group. According to a trial conducted by Dusunceli et al., there is a relationship between endurance capacity and cervical muscles strength on the neck pain. Exercises like stretching and isometrics serve to build muscular strength, restore damaged tissue, and support everyday activities.
In neck pain-affected individuals, static traditional stretching exercises were valuable to enhance the range of motion and alleviate pain. The various age factors in both the groups and the short-term use of long wave diathermy may be the cause of the insignificant variation in neck range of motion between the groups. Future studies may examine how individuals of similar ages respond to longwave diathermy. Studies may be carried out to determine the effectiveness of longwave diathermy on additional factors, such as the strength of the muscles in the neck, etc., and the long-term use of longwave diathermy as a therapy approach.
No limitations were reported.
Along with neck exercises, longwave diathermy intervention is beneficial to lessen neck disability and pain.
Journal of Physiotherapy Research
A randomized controlled trial on the efficacy of longwave diathermy on pain, disability and range of motion in the patients with neck pain
Usha Panihar et al.











Comments (0)