Categories
Change Password!
Reset Password!



In pediatric laparoscopic surgery, Magnesium sulfate and Dexmedetomidine plus Bupivacaine enhanced pain relief offered by Bupivacaine in the initial two postsurgery days.
In a prospective randomized clinical trial published in “Brazilian Journal of Anesthesiology”, preemptive intraperitoneal (IP) use of 0.5% Bupivacaine + Magnesium sulfate or Dexmedetomidine in hernia repair surgery offered better analgesic effectiveness compared to IP 0.5% Bupivacaine alone in pediatrics. This trial was purposed to investigate effectiveness of Magnesium sulfate or Dexmedetomidine with Bupivacaine in pediatric herniorrhaphy.
Overall, 97 male infants aged 1–6 years old and undergoing pediatric elective unilateral laparoscopic inguinal herniorrhaphy were randomly segregated to receive prior to peritoneal insufflation IP 2 mg/kg 0.5% Bupivacaine in combination with either 1 μg/kg of Dexmedetomidine (Group D), normal saline (Group C), or 30 mg/kg of Magnesium sulfate (Group M).
All medicines were diluted in normal saline to a volume of 10 mL. Within the first 48 hours following surgery, recording was done of Face, Legs, Activity, Cry, and Consolability (FLACC) pain ratings, the requisition for rescue analgesia, time to flatus and first stool, emetic episodes, side effects, functional recovery, and parental satisfaction.
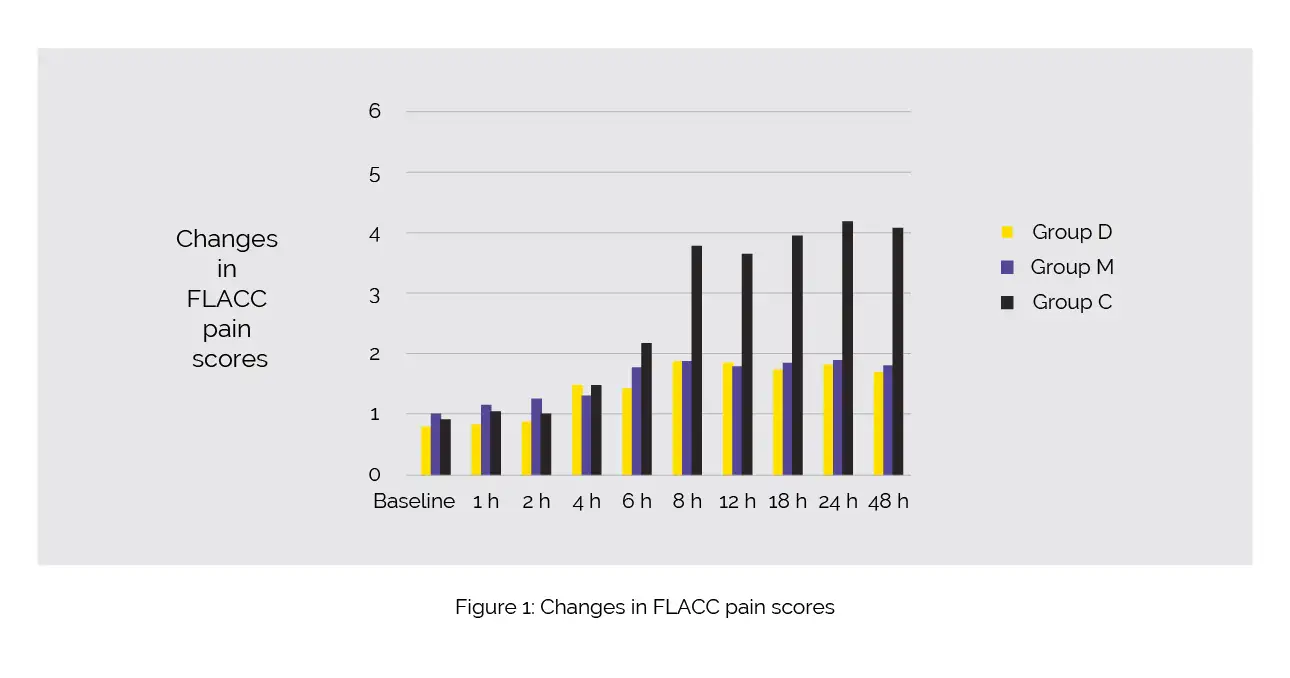
At 6, 8, 12, 18, 24, and 48 hours after surgery, Group C exhibited considerably elevated FLACC values when compared to Groups D and M. However, no differences were witnessed between Groups D and M, as shown in Figure 1:
The use of rescue analgesia was much greater in Group C, with no children in Groups D or M needing it. The time to first flatus and stool, emetic episodes, and unpleasant effects did not differ between the study groups. All groups had comparable times to recover to regular functional activities. Compared to Group C, parents were more satisfied in Groups M and D.
Therefore, the addition of Dexmedetomidine or Magnesium sulfate to Bupivacaine prior to peritoneal insufflation could be an ideal way for pain mitigation in children scheduled for herniorrhaphy with reduced analgesic usage, better gastrointestinal functions, and faster recovery.
Brazilian Journal Of Anesthesiology (English Edition)
Efficacy of dexmedetomidine versus magnesium sulfate as an adjuvant to intraperitoneal bupivacaine in pediatric laparoscopic surgery: a randomized clinical trial
Seham Mohamed Moeen et al.











Comments (0)