Categories
Change Password!
Reset Password!



Corticosteroids do not significantly reduce neonatal morbidity in early-term cesarean deliveries, so their use should be guided by the obstetrician's clinical judgment.
A new study published in Cureus questioned the necessity of administering antenatal corticosteroids before early-term cesarean sections, as researchers found no significant difference in neonatal outcomes between corticosteroid-treated groups and standard management. Infants born between 37 and 38 weeks +6 days via scheduled cesarean section, before labor, are at a higher risk of respiratory complications than those delivered between 39 and 40 weeks.
The benefits of antenatal corticosteroids before early-term cesarean sections are uncertain, with inconclusive evidence on reducing respiratory issues. This study by Namita Gupta et al. assessed the effectiveness and safety of intramuscular administration of Dexamethasone and Betamethasone phosphate in comparison to standard care for preterm newborns. After screening 241 pregnant women undergoing C-sections for eligibility criteria, 192 pregnant women undergoing early-term C-sections were considered and divided into three groups—receiving either Betamethasone, Dexamethasone or no corticosteroids (standard management protocol).
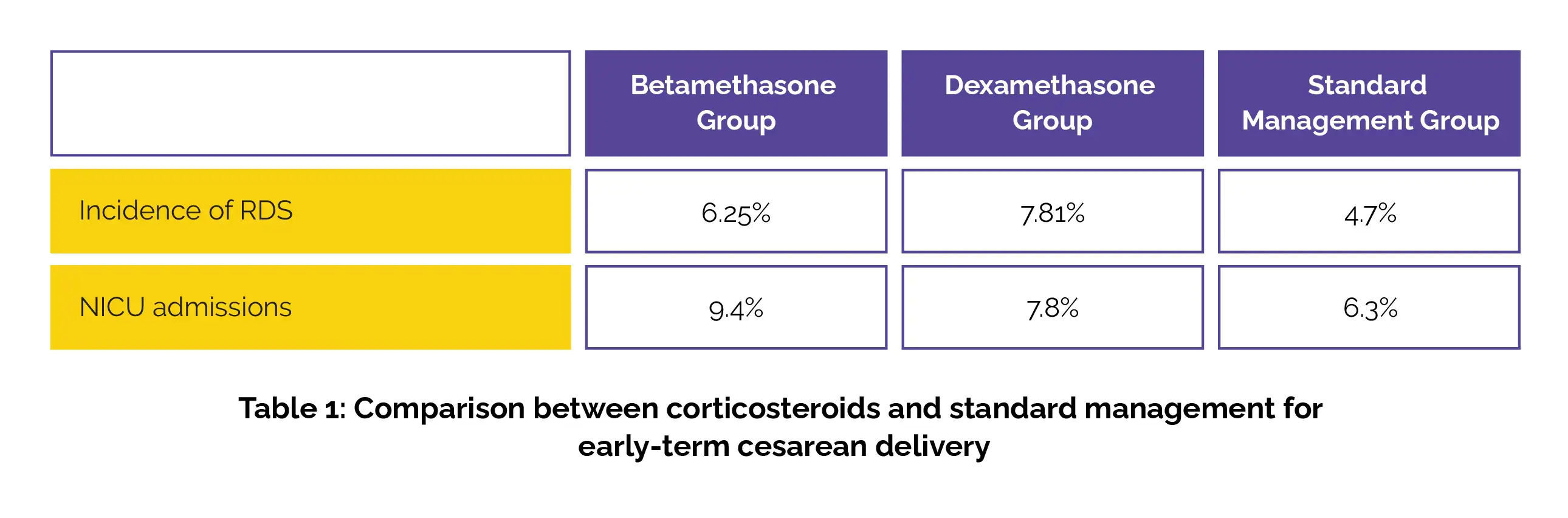
Researchers compared the rates of respiratory distress syndrome (RDS), transient tachypnea, and neonatal intensive care unit (NICU) admissions. The occurrence of RDS development did not differ considerably between the groups. Out of 192 infants, 15 required NICU admission for short stays (Table 1), and all improved with oxygen therapy without needing mechanical ventilation.
Hence, corticosteroid administration in early-term scheduled cesarean deliveries must be guided by the obstetrician's clinical judgment and individual patient factors.
Cureus
Comparative Study of the Safety and Efficacy of Intramuscular Dexamethasone, Betamethasone Phosphate, and Standard Management Protocol in Early-Term Scheduled Caesarean Delivery
Namita Gupta et al.













Comments (0)