Categories
Change Password!
Reset Password!


Nabumetone belongs to a class of drugs called nonsteroidal anti-inflammatory drugs (NSAIDs).
Nabumetone belongs to a class of drugs called nonsteroidal
anti-inflammatory drugs (NSAIDs). It is used primarily to reduce pain,
swelling, and joint stiffness from rheumatoid arthritis or osteoarthritis.
Pharmacological
class: NSAID
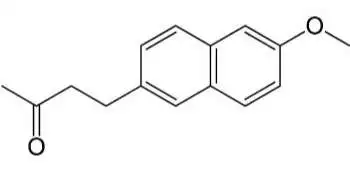
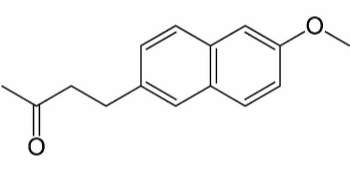
Nabumetone is a nonsteroidal
anti-inflammatory drug (NSAID) of the arylalkanoic acid family. Nabumetone is a
prodrug that upon hepatic catalysis converts into the active moiety
6-methoxy-2-naphthylacetic acid (6MNA). 6MNA inhibits the activity of the
enzymes cyclo-oxygenase I and II, resulting in decreased formation of
precursors of prostaglandins and thromboxanes. The resulting decrease in
prostaglandin synthesis is responsible for the therapeutic effects of
nabumetone.
Osteoarthritis
Rheumatoid Arthritis
Nabumetone is well absorbed from the GI tract and diffuses
readily into the synovia fluid. Nabumetone is metabolized to an active
metabolite 6-methoxy-2-napthylacetic acid (6-MNA) and inactive metabolites;
extensive first-pass effect; ~35% converted to 6MNA and 50% converted to
unidentified metabolites. The active metabolite is excreted in urine (80%) and
feces (9%).
Common (affecting between 1 in 10 to 1 in 100):
Uncommon (affecting 1 in 100 to 1 in 1000):
Very rare (affecting less than 1 in 10,000):
In a double blind,
randomized, parallel group study, 298 patients with rheumatoid arthritis received
nabumetone (2000 mg/day) or naproxen (1000 mg/day) for 3 months. At the end
point, nabumetone treated patients exhibited significant improvement in pain,
Ritchie articular index, and duration of morning stiffness when compared to
baseline. In contrast, naproxen treated patients showed significant improvement
only in Ritchie articular index. Nabumetone was significantly more effective
than naproxen for pain relief. Nabumetone was better tolerated than naproxen.1









Comments (0)