Categories
Change Password!
Reset Password!


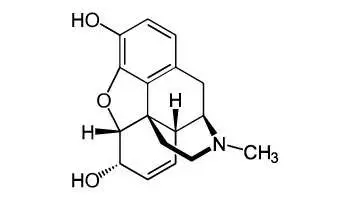
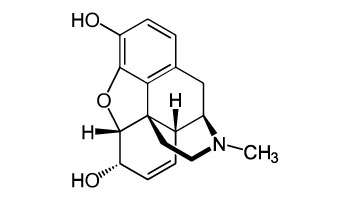
Morphine is a narcotic analgesic and it is available for administration as hydrochloride or sulfate salt in all dosage forms. It is a strong analgesic used primarily for the relief of severe pain.
Morphine is a narcotic analgesic and it is available for administration as hydrochloride or sulfate salt in all dosage forms. It is a strong analgesic used primarily for the relief of severe pain. Higher doses are useful for preoperative sedation and as a supplement to anesthesia. Morphine is also used for analgesia during labor. The effect on uterine contractions depends on the stage of labor when morphine is administered. Morphine is a drug of choice for pain associated with myocardial infarction.
Pharmacological Class: Opioid analgesic
The precise mechanism of the analgesic action of morphine is unknown. However, specific central nervous system (CNS) opiate receptors have been identified and likely play a role in the expression of analgesic effects. Morphine first acts on the µ-opioid receptors. The mechanism of respiratory depression caused by opioids involve a reduction in the responsiveness of the brain stem respiratory centers to increase in carbon dioxide tension and to electrical stimulation. It has been shown that morphine binds to and inhibits gamma-aminobutyric acid (GABA) inhibitory interneurons. These interneurons normally inhibit the descending pain inhibition pathway. So, without the inhibitory signals, pain modulation can proceed downstream.
Oral absorption of morphine is found to be 37.5%. Volume of distribution is found to be 2.75 l/kg and plasma protein binding is 30%. Presystemic metabolism is noted as 58% and metabolism occurs extensively by liver. Renal excretion accounts for 4% and plasma half life is 3 hours.
Common (affecting between 1 in10 to 1 in 100)
Uncommon (affecting 1 in 100 to 1 in 1000)
Very rare (affecting less than 1 in 10,000)










Comments (0)