Categories
Change Password!
Reset Password!


Dexlansoprazole is an FDA-approved new generation proton pump inhibitor (PPI) that is used for management of symptoms and lesions linked with erosive esophagitis and GERD.
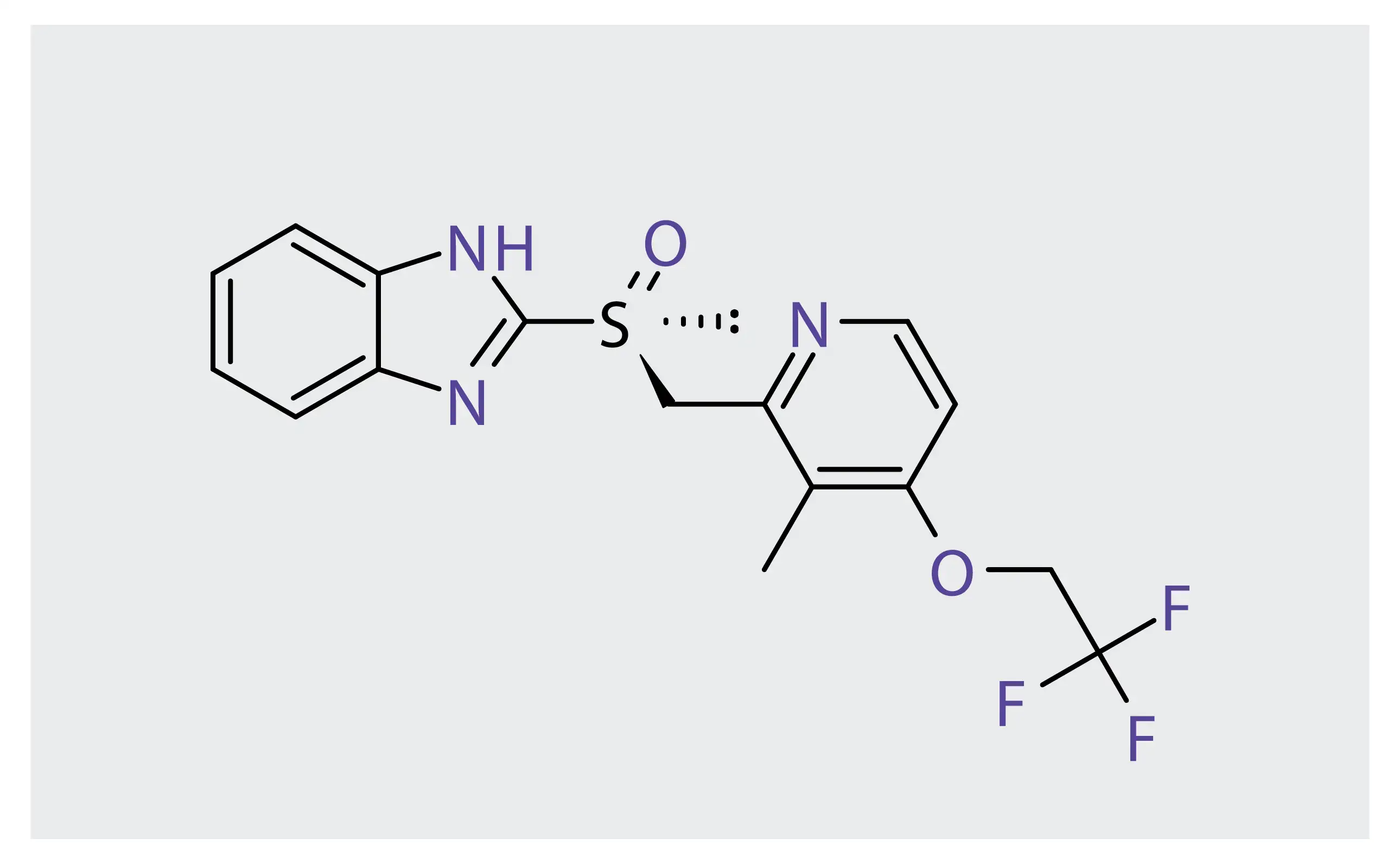
Dexlansoprazole is an FDA-approved new generation proton pump inhibitor (PPI) that is used for management of symptoms and lesions linked with erosive esophagitis and GERD. It is the R-enantiomer of lansoprazole, that is composed of a racemic mixture of R- and S-enantiomers. It is also used to treat H. pylori infection. [1,2]
In comparison with the older generation PPIs, this substituted benzimidazole prodrug with irreversible and selective proton pump inhibitor activity exhibits a unique pharmacokinetic profile due to its dual-delivery release and delayed-release system that addresses the limitations of older generation PPIs. [1]
Pharmacological Class: Proton pump inhibitor
It is indicated for:
The PPI dexlansoprazole leads to inhibition of hydrogen/potassium adenosine triphosphatase (H/K ATPase) enzyme. This enzyme is implicated in secretion of hydrochloric acid (HCl), hydrolyzing ATP and exchanging H+ ions from cytoplasm for K+ ions in the secretory canaliculus, that leads to secretion of HCl into gastric lumen. The PPI suppresses H/K ATPase's effect by illustrating a high degree of activation in acidic environment.
After passing through liver and reaching stomach parietal cells activated by a meal, dexlansoprazole undergoes protonation in acidic pH environment. This is subsequently followed by conversion to sulphenamide that represents drug's active form. Sulphenamide impedes activity of proton pump and hence transport of hydrogen ions into gastric lumen via covalent binding to SH groups of cysteine residues of the proton pump H/K ATPase.
Dexlansoprazole's delivery technology is designed to release the active ingredient in 2 separate pH-dependent phases. The 1st in proximal duodenum (25% of total drug dose is released at pH 5.5 ) and the 2nd (75% of total drug dose is released at pH 6.75) in the more distal small intestine. Dexlansoprazole leads to a reduction in both stimulated and basal secretion of gastric acid. [2,4]
Absorption
Following oral administration of dexlansoprazole, the peak plasma concentration rises approximately dose proportionally. The dual delayed-release formulation attains two plasma concentration peaks, where the 1st peak occurs 1-2 hours following administration. This is followed by a 2nd peak within 4-5 hours.
The median time (Tmax) to peak plasma concentrations (Cmax) of 30 mg dexlansoprazole was noted to be four hours. It ranged from one to six hours with Cmax value of 688 ng/mL. AUC was noted to be 3275 (ng∙h/mL).
Volume of distribution
Following multiple doses in symptomatic GERD people, the apparent volume of distribution in GERD people was 40.3 L.
Protein binding
In healthy subjects, dexlansoprazole's plasma protein binding ranged from 96% to 99% and was independent of concentration from 0.01 to 20 mcg/mL.
Metabolism
In liver, dexlansoprazole is substantially metabolized by reduction, oxidation, and subsequent formation of sulfate, glucuronide and glutathione conjugates to inactive metabolites. The formation of oxidative metabolites occurs with the aid of cytochrome P450 (CYP) enzyme system including hydroxylation primarily by CYP2C19, and oxidation to sulfone by CYP3A4.
Irrespective of CYP2C19 metabolizer status, dexlansoprazole is the primary circulating component in plasma. The principal plasma metabolites are 5-hydroxy dexlansoprazole and its glucuronide conjugate in CYP2C19 extensive and intermediate metabolizers. Dexlansoprazole sulfone is the chief plasma metabolite in CYP2C19 poor metabolizers.
Route of elimination
It is eliminated from the body by either renal excretion (47.6%) or fecal excretion (50.7%) after oral ingestion, without any unchanged drug detected in urine.
Half-life
It is eliminated with a half-life of approximately 1-2 hours in healthy subjects and in people with symptomatic GERD.
Clearance
Following 5 days of 30 or 60 mg once daily administration, dexlansoprazole's apparent clearance in healthy subjects was 11.4 to 11.6 L/hour. [1,2]
Dexlansoprazole is contraindicated in:
Dexlansoprazole should not be concomitantly administered with atazanavir because it may trigger a considerable drop in systemic concentrations of atazanavir.
Concomitant usage of tacrolimus might elevate whole blood concentrations of tacrolimus.
Dexlansoprazole might raise the serum levels of methotrexate.
Dexlansoprazole might impede the absorption of drugs (such as ketoconazole, ampicillin esters, iron salts, digoxin) for which gastric pH is crucial for bioavailability.
People taking concomitant warfarin may need monitoring for a rise in prothrombin time and international normalized ratio. [3]
The most commonly noted adverse reactions are:
(I) Dexlansoprazole for healing of erosive esophagitis and maintenance of healed erosive esophagitis
In a phase 2, multicenter, 36-week study, dexlansoprazole's dual delayed-release capsule was found safe and efficacious for healing erosive esophagitis and maintenance of healed erosive esophagitis in adolescents (12-17 years). This study was carried out to determine effectiveness and safety of dexlansoprazole in 62 adolescents with endoscopically confirmed erosive esophagitis. About 88% of people attained erosive esophagitis healing. During maintenance phase, the healing of erosive esophagitis was maintained in 58% and 82% of placebo and dexlansoprazole groups, respectively. [5]
(II) In patients with heartburn
An open-label trial was carried out to determine the efficacy of 60 mg dexlansoprazole in 32 people with symptomatic heartburn. The major outcome was heartburn alleviation defined as mean 24-h free heartburn percentage per weekly period. During the first week, only one person (3.1%) was heartburn-free and mean 24-hour free heartburn percentage was 41.1 ± 24.8%. Following dexlansoprazole initiation, the mean 24-hour free heartburn percentage elevated to 63.4 ± 23.8 and 81.6 ± 24.5% in second and fourth week, respectively.
The median 24-hour free heartburn percentage elevated from 35.7% in first week to 71.4 and 85.7% in second and fourth weeks, respectively. The Mean Gastroesophageal Reflux Disease Questionnaire (GERDQ) scores dropped from 10.0 ± 3.2 in week 1 to 6.53 ± 2.2 in week 2 and 5.87 ± 2.1 in week 4. Furthermore, the mean heartburn severity score dropped from 2.5 ± 1.0 to 1.7 ± 0.8. Early response was greater in people with GERDQ scores ≥8. Dexlansoprazole was found effective to treat heartburn. [6]
In another placebo-controlled, double-blind, four-week study, dexlansoprazole modified release 30 and 60 mg showed good tolerability and were superior to placebo in providing 24-hour heartburn-free days and nights in people with non-erosive reflux disease. [7]
(III) In patients with H. pylori infection
In a prospective randomized trial, dexlansoprazole modified release-based concomitant therapy (as a first-line H. pylori treatment regimen) achieved a successful H. pylori elimination rate of 90%, that was non inferior to that of lansoprazole-based concomitant therapy. [8] Another trial was carried out to determine the effectiveness of dexlansoprazole for H. pylori elimination as triple therapy in real-world practice. Dexlansoprazole-based triple therapy exhibited an acceptable elimination rate for H. pylori infection. [9]
In another pilot, randomized, controlled study, a single-dose dexlansoprazole modified release-based triple therapy was found to offer a similar elimination rate as double-dose rabeprazole-based therapy in people with H. pylori infection. [10]











Comments (0)