Categories
Change Password!
Reset Password!


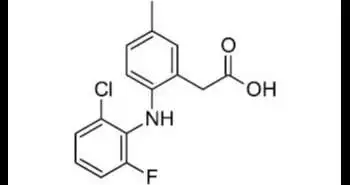
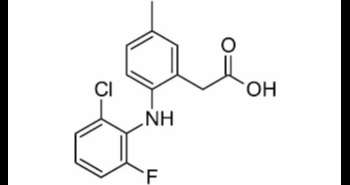
Lumiracoxib is a
COX-2 selective inhibitor non-steroidal anti-inflammatory drug.
Lumiracoxib is a COX-2 selective inhibitor
non-steroidal anti-inflammatory drug. It belongs to the class of organic
compounds known as phenylacetic acid derivatives. It is widely used in the
treatment of patients suffering from osteoarthritic pain
Pharmacological class: NSAID
The mechanism of action of lumiracoxib involves the
inhibition of prostaglandin synthesis via inhibition of cyclo-oxygenase-2
(COX-2) enzyme. Lumiracoxib does not inhibit COX-1 at therapeutic
concentrations.
Osteoarthritis:
100 to 400 mg orally per day
Rheumatoid arthritis:
200 to 400 mg orally per day
Lumiracoxib is rapidly absorbed, achieves mean plasma
concentrations >1 microg/ml within 1 h of dosing. Unchanged drug in plasma
accounts for 81 to 91% of radioactivity up to 2.5 h post dose, suggesting a
modest first-pass effect; unchanged drug is the major circulating component in
plasma, accounting for approximately 43% of AUC (0 to 24 h). The terminal
half-life of lumiracoxib in plasma is found to be 6.5 h. Major plasma
metabolites are the 5-carboxy, 4'-hydroxy, and 4'-hydroxy-5-carboxy
derivatives. Excretion involves both renal (54.1%) and fecal (42.7%) routes,
and dose recovery is almost complete (96.8%). It is extensively metabolized
before excretion, with little unchanged drug in urine (3.3% of dose) or feces
(2.0% of dose).
Common (affecting between 1
in10 to 1 in 100):
Uncommon (affecting 1 in 100 to 1 in 1000):
Very rare (affecting less than 1 in 10,000):
In a 13-week, multicenter,
randomized, double-blind, double-dummy, placebo-controlled study, males or
females aged >/= 18 years with primary knee OA received lumiracoxib 100 mg
od, lumiracoxib 100 mg od with a loading dose of 200 mg od for the first two
weeks, celecoxib 200 mg od, or placebo. All active treatments were superior to
placebo for all co-primary variables. No significant differences were observed
between any active treatments. Mean reductions from baseline to week 13 for
lumiracoxib 100mg od, 100mg od with loading dose, celecoxib and placebo,
respectively, were: OA pain intensity in the target knee: 26.8, 26.2, 26.6 and
21.4mm (all p < 0.01 vs. placebo); patient's global assessment of disease
activity: 25.1, 21.9, 22.9 and 18.9 mm (all p < 0.05 vs. placebo); WOMAC
total score: 15.2, 14.8, 14.7 and 11.3 (all p < 0.01 vs. placebo).
Lumiracoxib was superior to placebo and similar to celecoxib for OMERACT-OARSI
response and WOMAC subscale scores. Lumiracoxib was well tolerated.1










Comments (0)