Категории
Сменить пароль!
Сброс пароля!


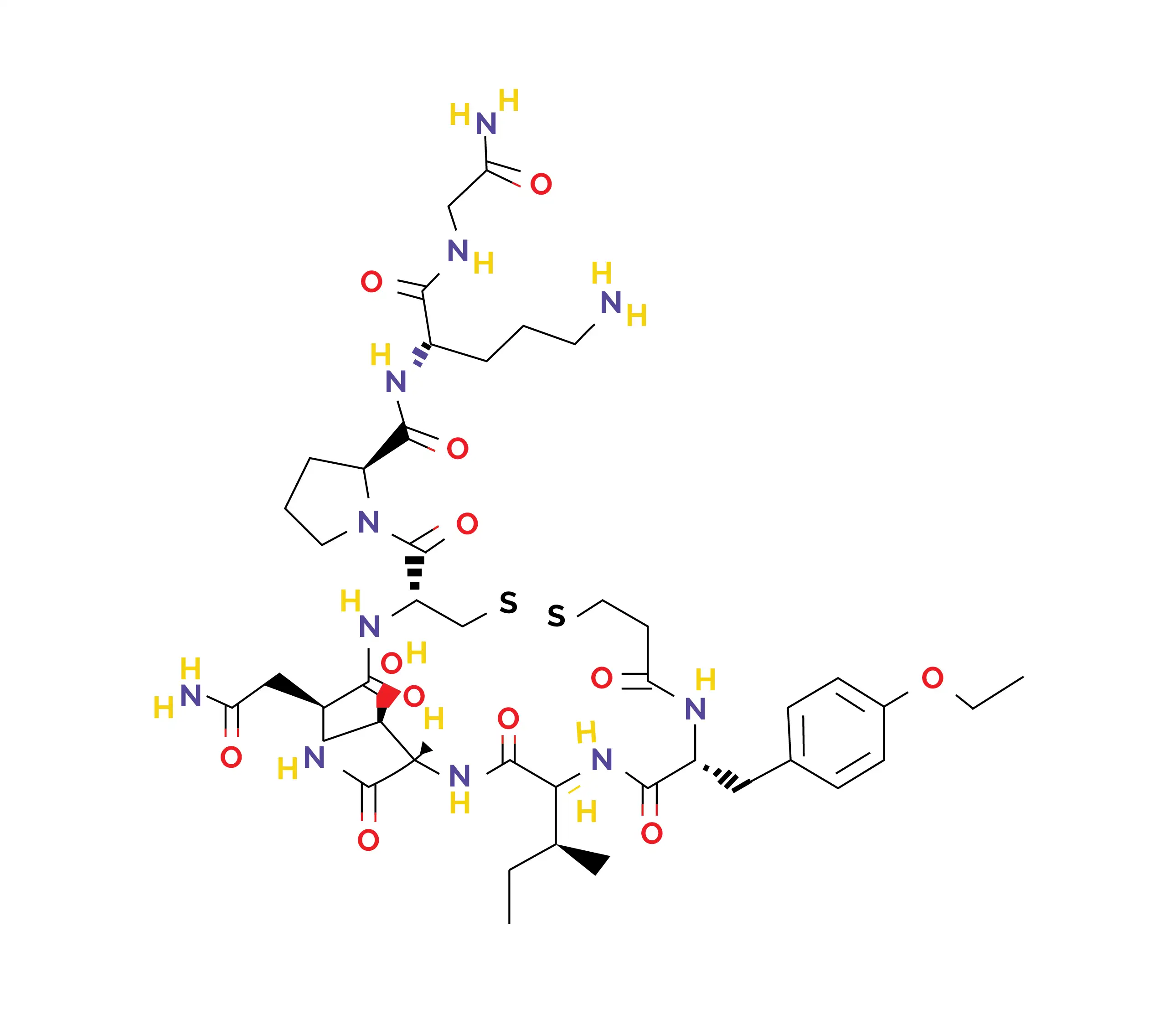
Атозибан — это олигопептид, который ингибирует гормоны окситоцин и вазопрессин.
Атозибан — это олигопептид, который ингибирует гормоны окситоцин и вазопрессин. Его вводят внутривенно для предупреждения преждевременных родов (родов, наступающих на сроке до 37 недель беременности) [1, 2]. Он доступен на рынке в виде запатентованного препарата и воспроизведенных препаратов (дженериков) и одобрен для применения у беременных женщин при риске неизбежных преждевременных родов, установленном на основании определенных клинических наблюдений [2].
Химическая формула: C43H67N11O12S2
Атозибан показан для отсрочки неизбежных преждевременных родов у беременных женщин, у которых наблюдаются следующие признаки:
(a) регулярные сокращения матки продолжительностью не менее 30 секунд, повторяющиеся с частотой четыре или более раз в течение 30 минут;
(b) раскрытие шейки матки на 1–3 см (0–3 см для ранее не рожавших женщин) и сглаживание (истончение и укорочение шейки матки, которое происходит во время беременности при подготовке к родам) не менее 50 %;
(c) срок беременности от 24 до 33 полных недель;
(d) нормальная частота сердечных сокращений плода [2].
Атозибан можно применять для повышения частоты успешного экстракорпорального оплодотворения и переноса эмбрионов (ЭКО-ПЭ) [3]. Особенно рекомендуется его применение у женщин старшего возраста и женщин с ожирением в случае повторных неудачных попыток имплантации во время циклов переноса свежих эмбрионов [4].
Система окситоцина, которая действует через рецепторы окситоцина в матке, имеет основополагающее значение для родовой деятельности у человека. Повышенная экспрессия рецепторов окситоцина играет основную роль в индукции преждевременных родов. В молекуле атозибана, аналога окситоцина, аминокислоты в положении 1, 2, 4 и 8 были изменены. Атозибан конкурирует с окситоцином за связывание с его рецепторами, что приводит к снижению интенсивности сокращений миометрия [5]. Это предупреждает вызванное окситоцином повышение уровня инозитолтрифосфата, который отвечает за стимуляцию сокращений.
Это действие, в свою очередь, предотвращает высвобождение накопленного кальция из саркоплазматического ретикулума и открытие потенциал-чувствительных кальциевых каналов. В результате ограничивается повышение уровня цитозольного кальция, что предотвращает сокращения мышц матки, снижает их частоту и вызывает состояние покоя матки (состояние матки, при котором отсутствуют скоординированные сокращения). В ходе недавних исследований было установлено, что атозибан также действует как лиганд, изменяющий функцию рецепторов окситоцина. Он является антагонистом связывания с Gq-белком, что объясняет его ингибирующее влияние на путь инозитолтрифосфата, который, как полагают, опосредует его влияние на сокращения матки.
И наоборот, атозибан действует как агонист связывания с Gi-белком, приводя к провоспалительному ответу в амнионе человека за счет активации транскрипционного фактора каппа B (NF-κB), трансдуктора передачи провоспалительных сигналов. Считается, что такая провоспалительная активность снижает эффективность атозибана по сравнению с другими лекарственными средствами, не вызывающими воспаления, поскольку известно, что медиаторы воспаления способствуют индукции родов [2]. В случае применения при преждевременных родах атозибан быстро подавляет сокращения матки. Уже через 10 минут после введения он значимо снижает сократительную активность, способствуя поддержанию стабильного состояния функционального покоя матки до 12 часов [6].
Атозибан вводят сразу же после постановки диагноза «преждевременные роды».
Дополнительные аспекты
Абсорбция
Распределение
Метаболизм
Выведение
(a) По ведению преждевременных родов
(b) По профилактике преждевременных родов при беременности двойней
(c) По улучшению исходов беременности у женщин с неудачными попытками имплантации эмбриона в ходе ЭКО
1. Atosiban. PubChem. Доступно по ссылке: https://pubchem.ncbi.nlm.nih.gov/compound/Atosiban. PubChem CID: 5311010.
2. Atosiban, Drug Bank. Доступно по ссылке: https://go.drugbank.com/drugs/DB09059. Инвентарный номер: DB09059.
3. Wang R, Huang H, Tan Y, Xia G. Efficacy of atosiban for repeated embryo implantation failure: A systematic review and meta-analysis. Frontiers in Endocrinology (Lausanne). 2023 Mar 23;14:1161707.
4. Li J, Mo S, Lin Z, Shi Q. Atosiban application in fresh ET cycle is effective for women undergoing repeated embryo implantation failures, especially for advanced-age obese patients. Scientific Reports. 2023 Dec 27;13(1):23044.
5. Dewan B. Oxytocin Antagonist Atosiban for the Treatment of Preterm Labor: Clinical Trial Evidence. London Journal of Medical and Health Research. 2024 Feb 7;24(1):35-45.
6. Atosiban. Vidal. Доступно по ссылке: https://www.vidal.ru/drugs/atosiban
7. Atosiban. Summary of Product Characteristics. Доступно по ссылке: https://www.ema.europa.eu/en/documents/product-information/atosiban-sun-epar-product-information_en.pdf
8. Dewan B, Shinde S. Clinical safety and efficacy of atosiban brief duration 14-hour treatment regimen in delaying preterm labor. International Journal of Reproduction, Contraception, Obstetrics and Gynecology. 2023;12(6):1862-5.
9. Al-Riyami N, Al-Badri H, Jaju S, Pillai S. Short-Term Outcomes of Atosiban in the Treatment of Preterm Labour at the Sultan Qaboos University Hospital, Muscat, Oman: A tertiary care experience. Sultan Qaboos University Medical Journal. 2021 May;21(2):e260-e265.
10. Romero R, Sibai BM, Sanchez-Ramos L, Valenzuela GJ, Veille JC, Tabor B et al. An oxytocin receptor antagonist (atosiban) in the treatment of preterm labor: a randomized, double-blind, placebo-controlled trial with tocolytic rescue. American Journal of Obstetrics & Gynecology. 2000 May;182(5):1173-83.
11. Mariavittoria L, Giovanni N, Marilena M, Raffaella I, Emilia S, Teresa P et al. Two cycles of Atosiban in preventing preterm birth in twin pregnancies. Clinical Obstetrics, Gynecology and Reproductive Medicine. 2016;2(4):221-4.













Комментарии (0)